Gastrointestinal Stromal Tumor (GIST)
58 y/o F no PMH with epigastric pain for two days, nausea and generalized weakness but no other symptoms. Vital signs were normal and physical exam was limited due to obesity but revealed moderate tenderness in the epigastric region without distention or peritoneal signs. The remainder of the exam was unremarkable and POCUS was performed.
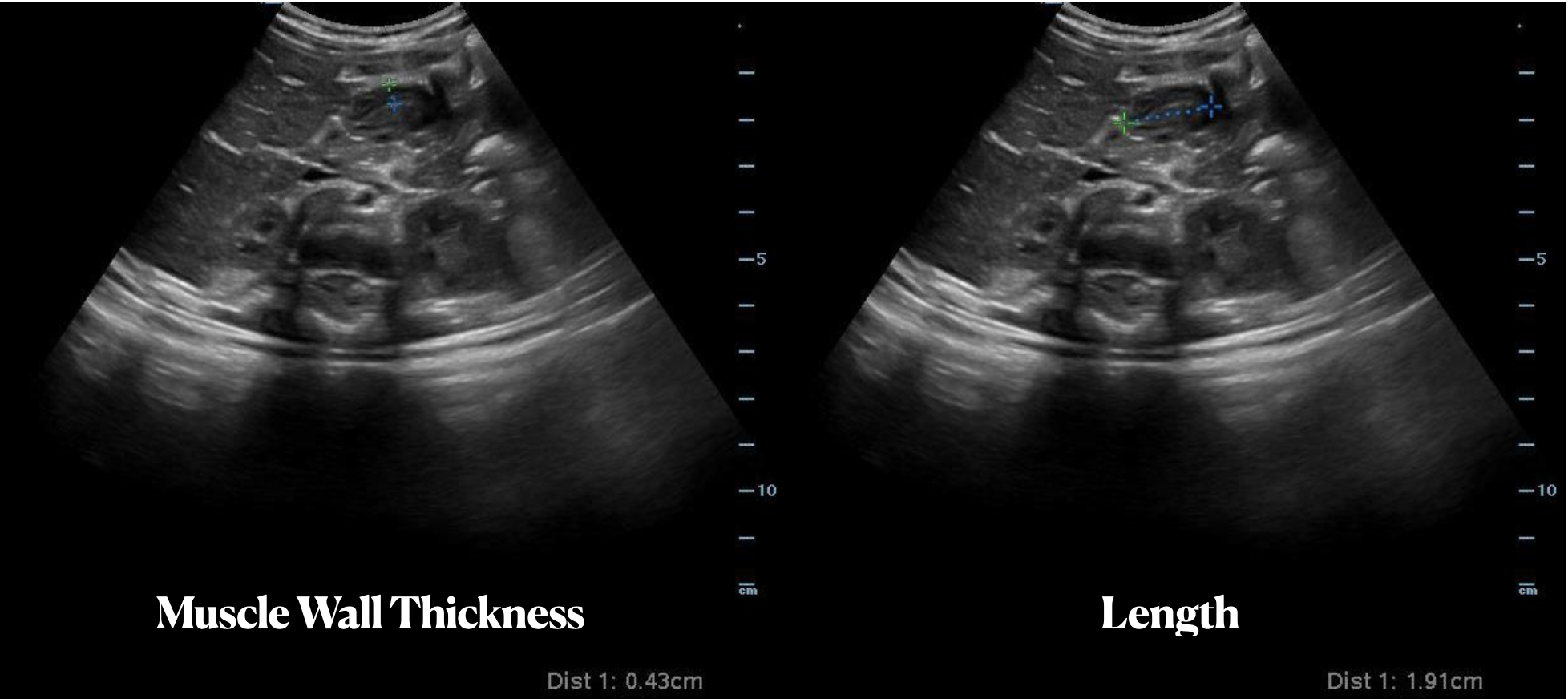
A subcostal view is above showing an undefined hypoechoic, heterogeneous, cystic mass. It was non-compressible with well defined borders.
Computed tomography (CT) of the abdomen and pelvis confirmed a large, heterogeneous mass adjacent to the stomach with a small amount of intra-abdominal and intra-pelvic blood. The patient was admitted to general surgery, and endoscopic ultrasonography with biopsy revealed a spindle cell lesion consistent with gastrointestinal stromal tumor (GIST).
Gastrointestinal stromal tumors are the most common mesenchymal tumors of the GI tract with an incidence of 14 to 20 cases per million.(1) They can be located anywhere in the GI tract but are most frequently identified in the stomach (50-60%) and small bowel (30-40%).(2) Symptoms include abdominal pain, nausea, dyspepsia, fatigue, constipation, or diarrhea. Gastrointestinal stromal tumors have varying appearance on different imaging modalities and are often first seen on abdominal ultrasonography.(3)
A subcostal view is be a good place to begin POCUS, considering that most GISTs are located adjacent to or within the stomach. Case reports describe the diagnosis of GIST with help of initial transabdominal ultrasonography.(4,5) Appearance on ultrasonography may vary, depending on size and mitotic activity.(3) Larger tumors may often appear as heterogeneous masses, filling the abdomen with hypoechoic areas consistent with necrosis.(1) However, reports also describe tumors initially seen as extraluminal hypoechoic masses of varying size.(5)
While transabdominal ultrasonography is an excellent starting point, CT ultimately shows better detail for staging and characterization. Endoscopic ultrasonography can be used for further definition and ultimately for diagnosis, as biopsy is required.
Point-of-care ultrasonography may be an excellent tool for determining further management of patients with non-specific abdominal symptoms. While you may not initially suspect a GIST when starting your POCUS, an unidentifiable mass in the GI tract should prompt further investigation, which can ultimately lead to formal diagnosis.
References
Vernuccio F, Taibbi A, Piccone D, et al. Imaging of Gastrointestinal Stromal Tumors: From Diagnosis to Evaluation of Therapeutic Response. Anticancer Research 2016;36(6):2639–48.
Wronski M, Cebulski W, Slodkowski M, Krasnodebski I. Gastrointestinal Stromal Tumors . Journal of Ultrasound 2009;28(7):941–8.
King DM. The radiology of gastrointestinal stromal tumours (GIST). Cancer Imaging 2005;5(1):150–6.
Sugihara T, Koda M, Tanimura T, Yoshida M, Muruwaki Y. A report of three cases of exophytic gastrointestinal stromal tumor detected by transabdominal ultrasound. Journal of Medical Ultrasonics 2016;43(1):107–11.
Chan KP. What’s the Mass? The Gist of Point-of-care Ultrasound in Gastrointestinal Stromal Tumors. Clinical Cases and Reports in EM 2018;2(1).