This was a prospective observational study comparing the operating characteristics of emergency department (ED) performed LUS versus CXR for the diagnosis of pneumonia in patients with suspected H1N1 influenza. The operating characteristics described in the table include patients with any pneumonia: primary bacterial pneumonia, viral (H1N1) pneumonia, or a secondary bacterial pneumonia in H1N1 infected patients. Patients were included in the experimental arm if they had signs or symptoms of influenza-like illness (ILI) with suspicion of lung involvement (pneumonia), either bacterial or viral. A total of 87 patients were enrolled in the study, 41 with ILI with suspected pneumonia and 46 with ILI without suspected pneumonia (control group).
The gold standard final diagnosis of pneumonia was based on the chart review of the hospital course including the history, physical exam, lab results, and radiographic findings. The reviewers were blinded to the LUS results. Three outcomes were reported: viral pneumonia with laboratory confirmation of the H1N1, primary bacterial pneumonia, or secondary bacterial pneumonia with confirmed H1N1.
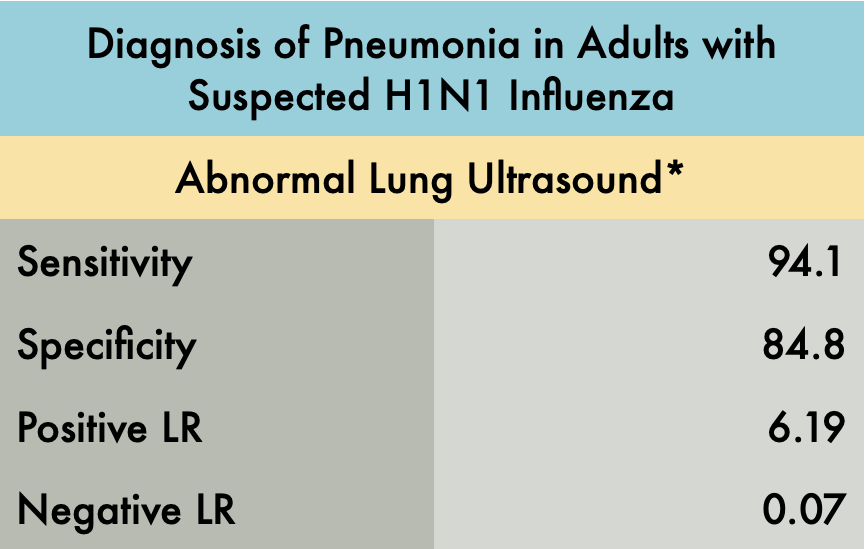
The LUS studies were performed by three different emergency physicians with greater than 10 years of ultrasound experience. This study evaluated each hemithorax in five areas: two anterior, two lateral, and one posterior. The presence of any of the following signs on LUS indicated an abnormal exam*:
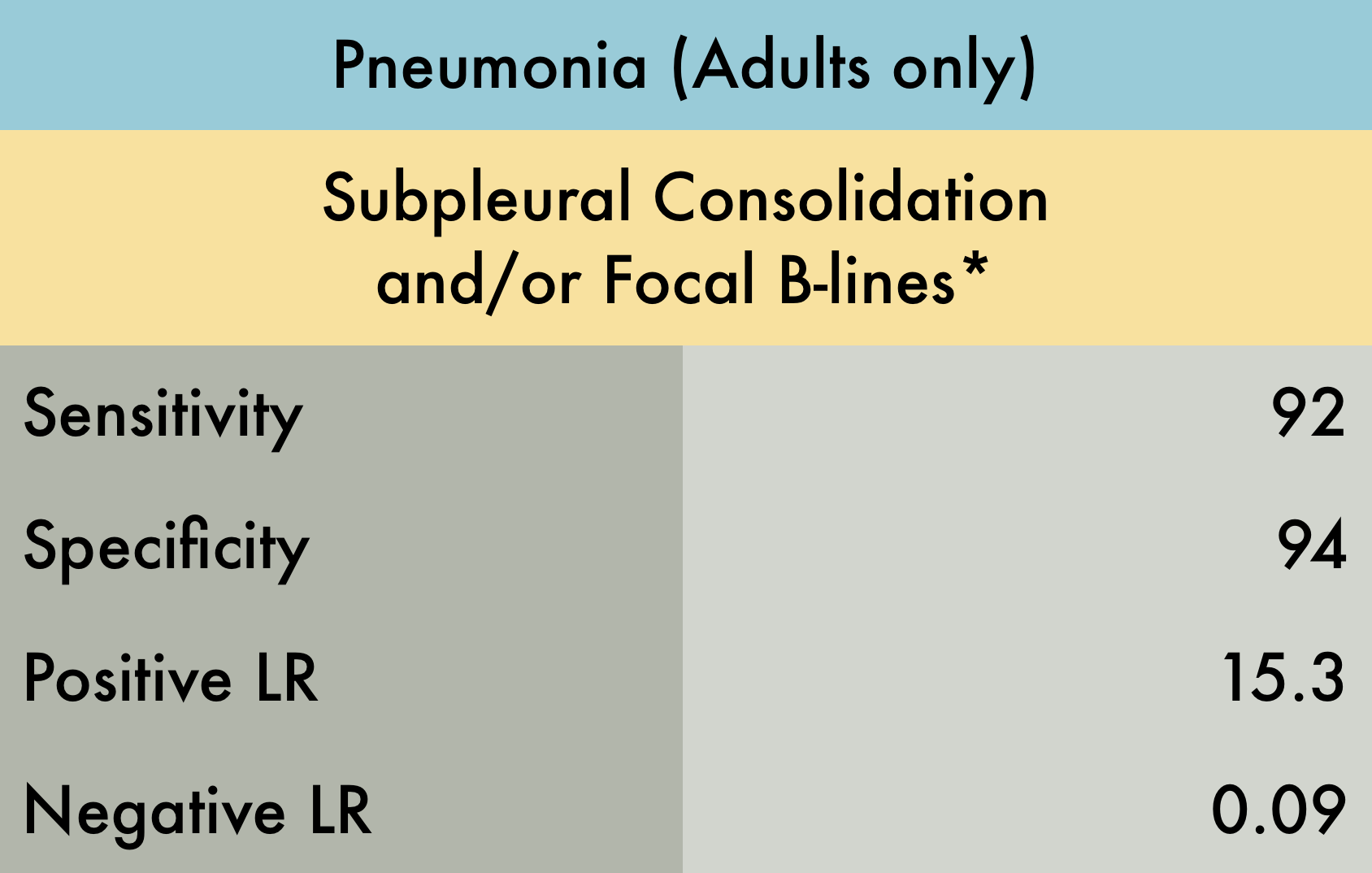
>3 B-lines per intercostal space
Thickness of pleural line > 2mm or coarse appearance
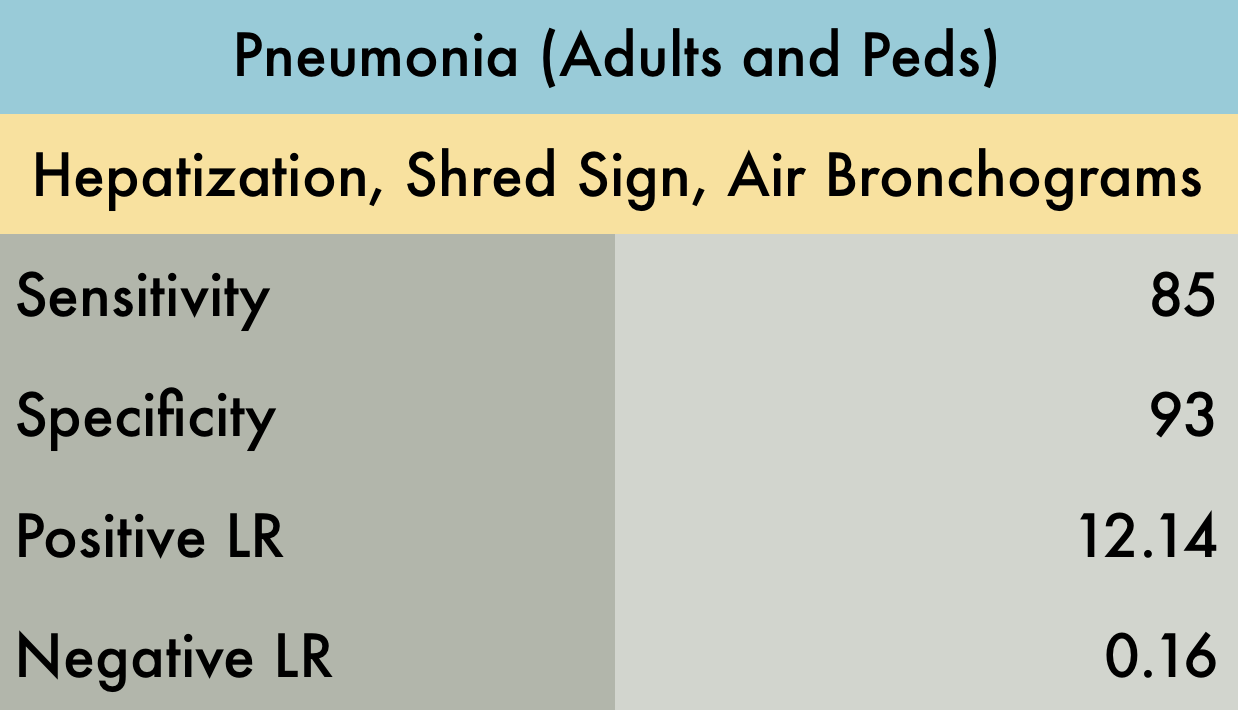
Consolidation or hepatization
Pleural effusion
Lung ultrasound showed a sensitivity of 94.1% and specificity of 84.8%. An abnormal ultrasound was present in 32 of 34 patients with the ultimate diagnosis of pneumonia (including viral and bacterial). In patients with initially negative CXRs, 15/16 demonstrated an US pattern reflecting interstitial syndrome, all of whom ultimately had the diagnosis of pneumonia. In patients with initial abnormal CXRs, 17/18 had positive chest ultrasounds. The control arm did have 5/33 false positives which the author speculates may have been attributed to subclinical viral infections without clinical relevance or previous interstitial syndromes reflecting priorillness. The one false negative case was a patient with bacterial pneumonia with a deep, perihilar opacity.
The main limitation of this study is the small sample size and that the LUS studies were performed by expert sonographers. Beyond this though, we recognize that this study identified operating characteristics of LUS for all pneumonia and did not specifically analyze the sensitivity and specificity of lung ultrasound for viral pneumonia alone. It also excluded patients with comorbidities making this a very limited patient population which likely greatly affected the specificity of POCUS for pneumonia in this setting. Furthermore, expert adjudication was used to determine final diagnosis which is an imperfect gold standard. In the end, H1N1 has many similar characteristics to the COVID pandemic and this study is highly suggestive that lung ultrasound, particularly in patients with negative CXRs, can assist in diagnosis.
PMID: 22340202