ddxof: Ultrasound in Ectopic Pregnancy
Another #FOAMEd knowledge bomb from our partner ddxof
Check out the original post here: ddxof: Ultrasound in Pregnancy
This would make a great intro for any GYN ultrasound student learner, or even third year medical student in OBGYN. We will paraphrase here but be sure to check out the original post for the evidence based details.
From their post: 27 year old female syncopizes, comes in from EMS hypotensive. She is lethargic and has a remarkably tender abdomen. You perform your rush exam, starting with a FAST which shows free fluid. HCG is positive. Large bore IV's, uncrossmatched blood, and get them to the OR with GYN STAT.
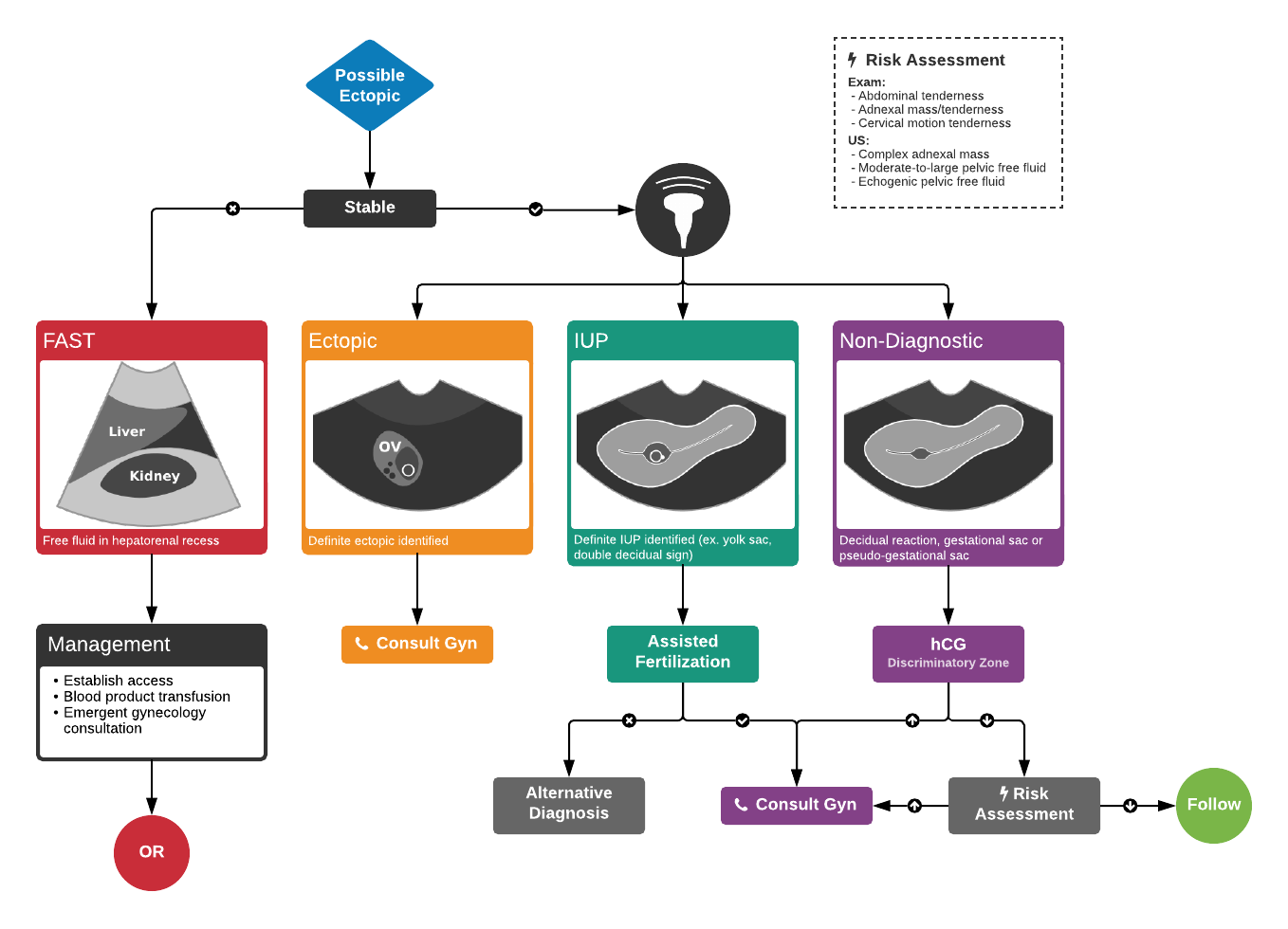
Algorithm for the Evaluation of Suspected Ectopic Pregnancy
What do these things look like on ultrasound? That is where our GYN Atlas comes in. Here are some of our favorite ectopic images hand picked for you.
Featured