ddxof: POCUS for Undifferentiated Shortness of Breath
Undifferentiated Shortness of Breath

This is a co-post with our FOAMEd partner The ddxof - project of Dr. Tom Fadial . ddxof: is a compilation of cases based on real patients, each inspiring an algorithm for the evaluation and management of their chief complaint or diagnosis.
If you have any ideas for collaborating with our team don't hesitate to reach out.
Please see the original post here https://ddxof.com/ultrasound-in-dyspnea/
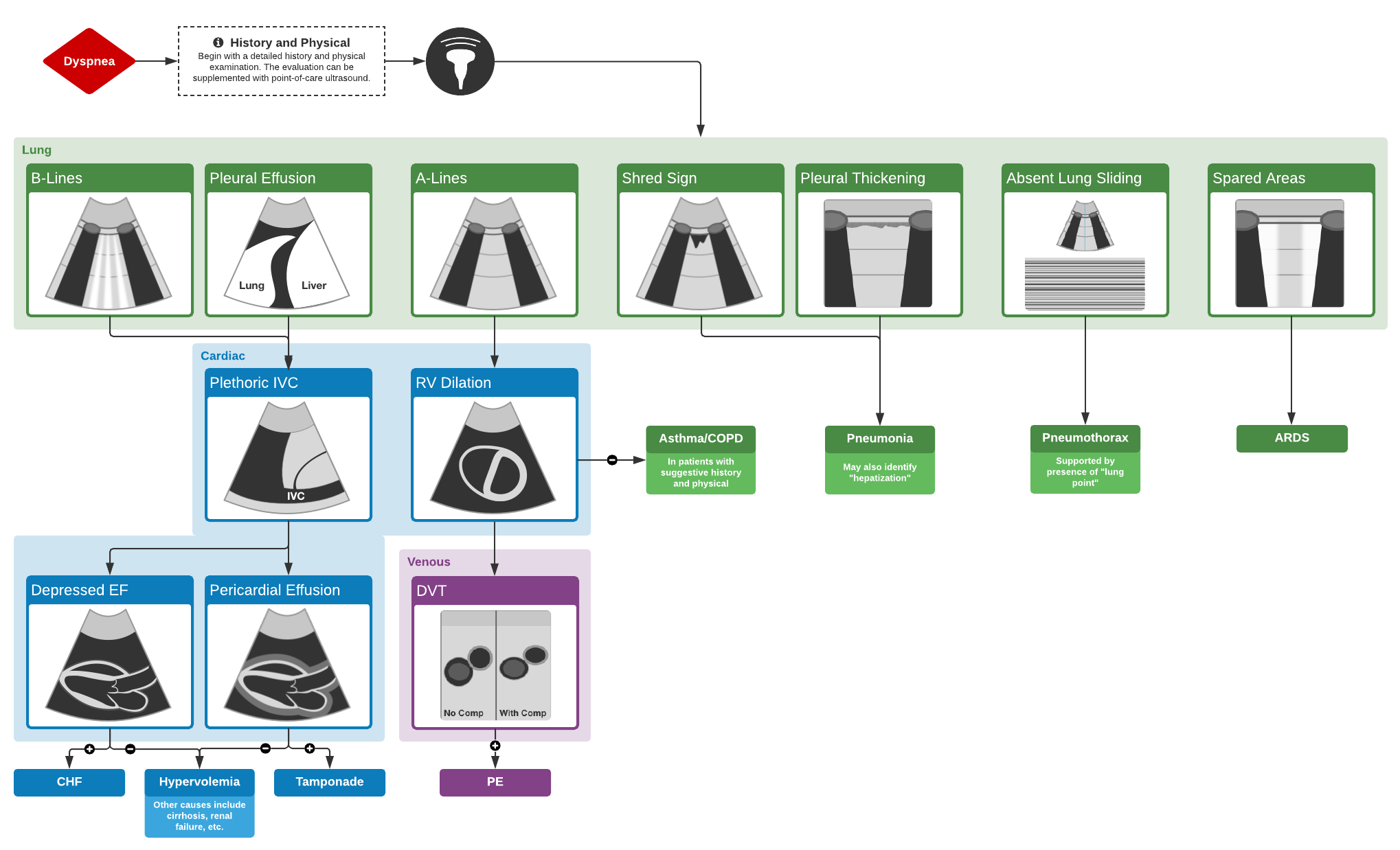
This is a common emergency department scenario: a critically-ill patient with undifferentiated dyspnea. The physical exam can be difficult and indeterminate with huge risks of deterioration. Our CHF patients often have COPD, afib and maybe renal failure. Your decisions matter. Here is a proposed approach for these patients.
Algorithm for the Use of Ultrasound in the Evaluation of Dyspnea
Featured