The Evidence Atlas: Echocardiography
Jump To Clinical Application: Heart Failure Pulmonary Embolism Cardiac Arrest
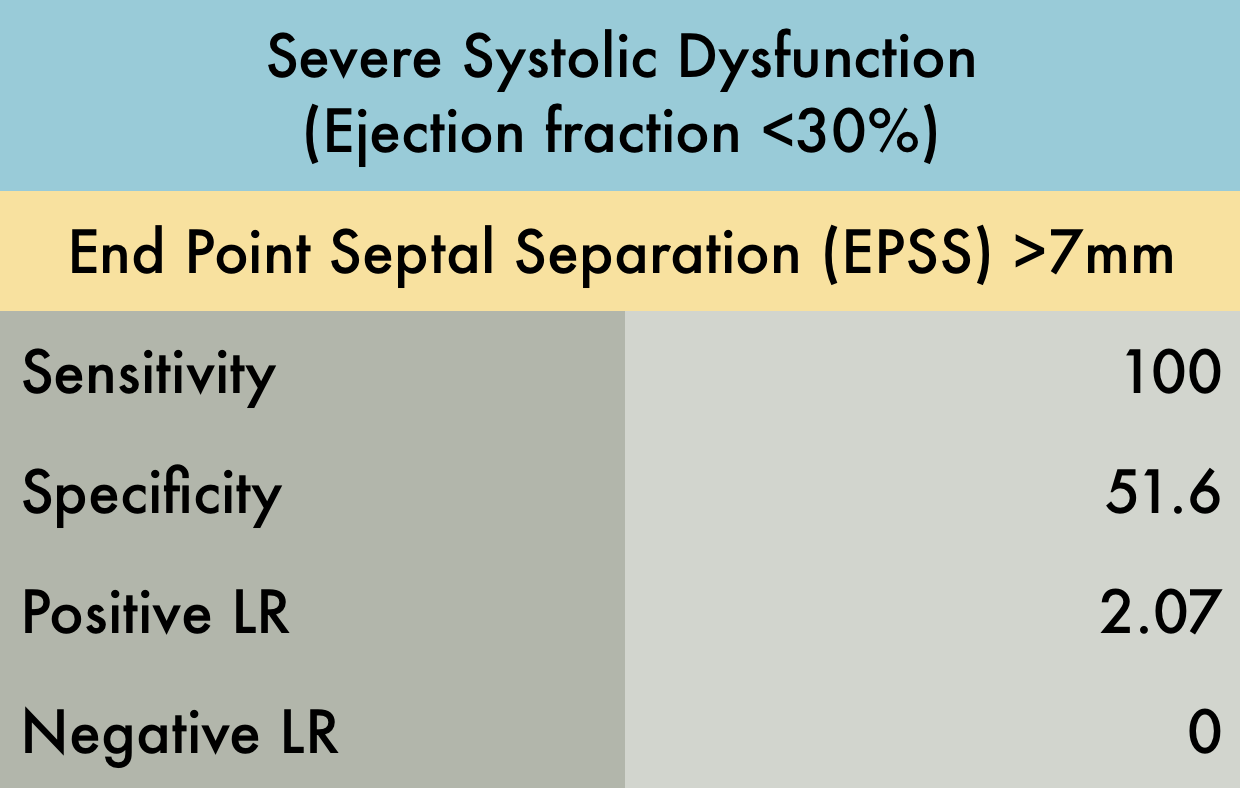
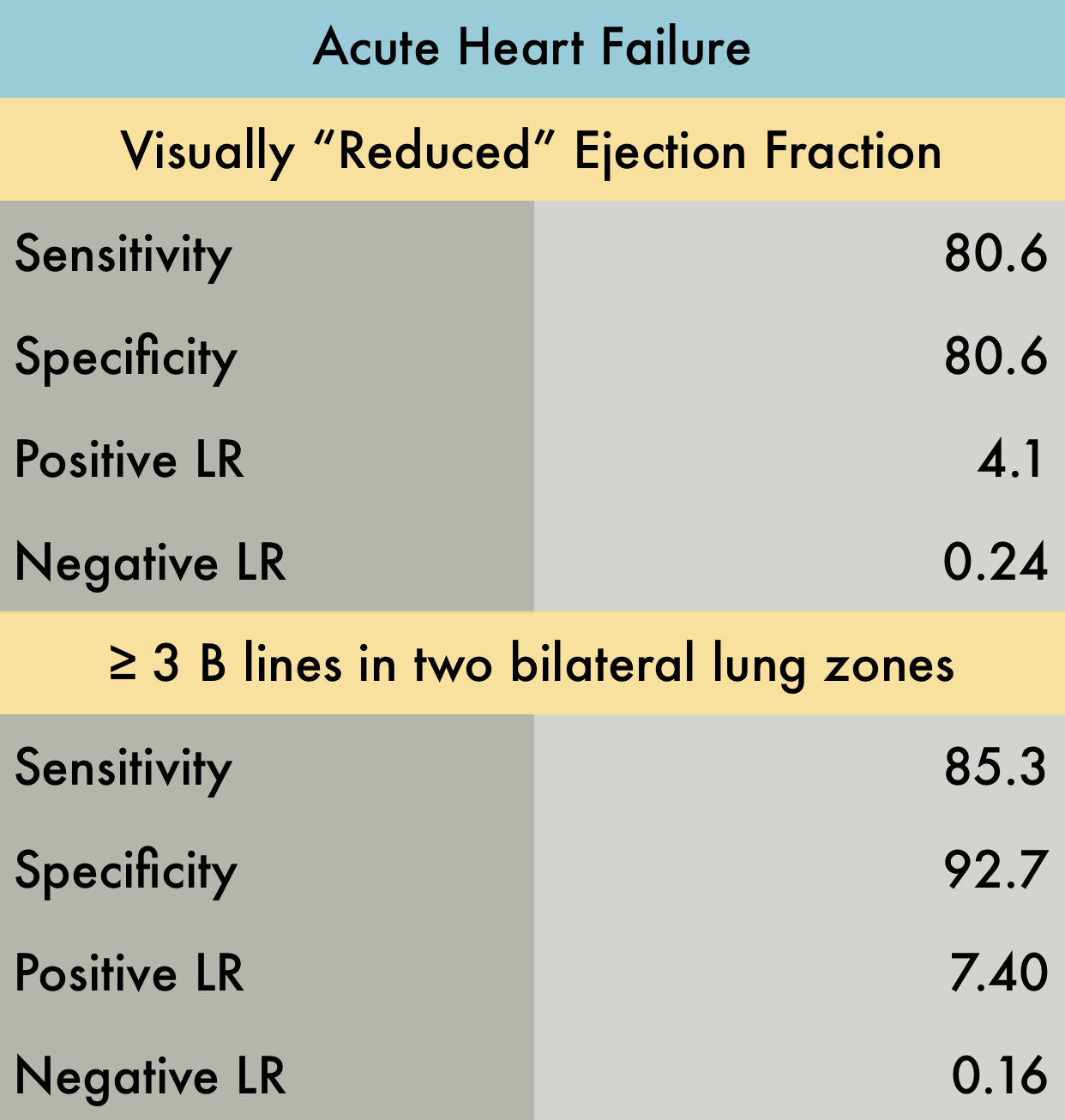
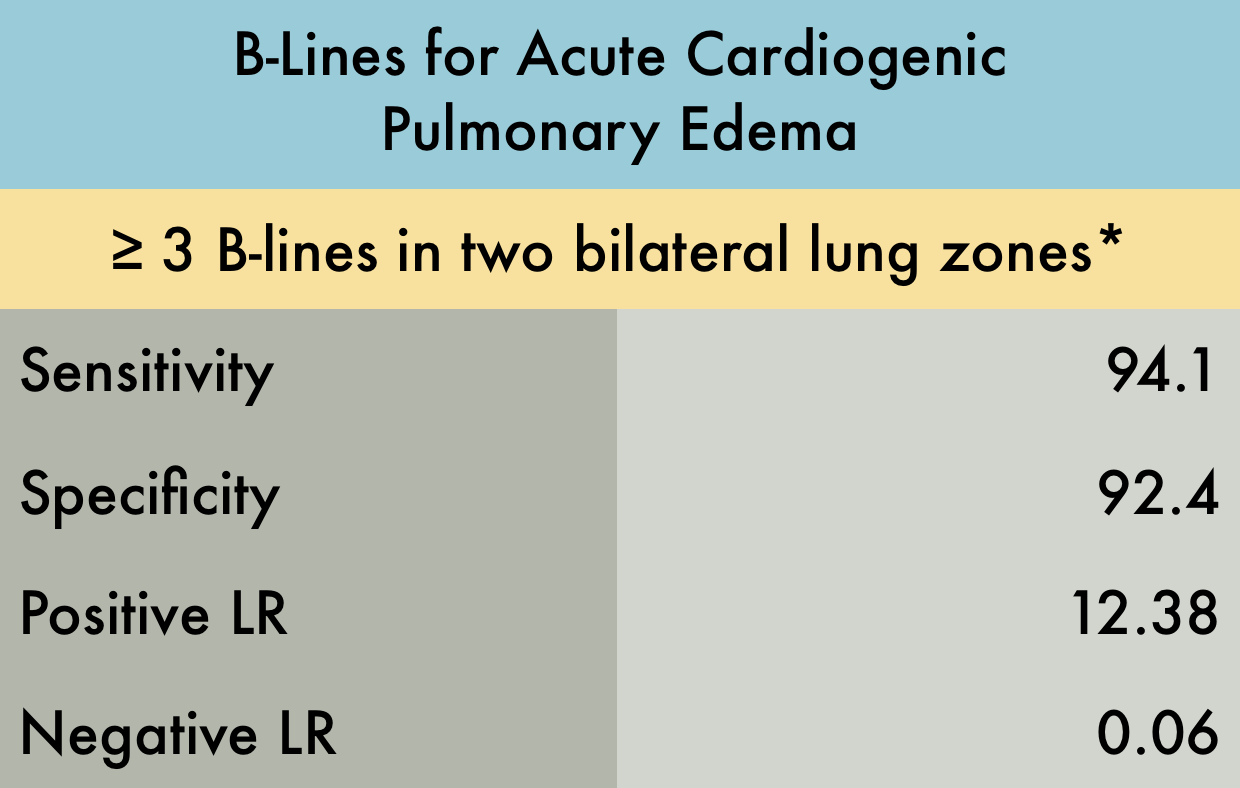
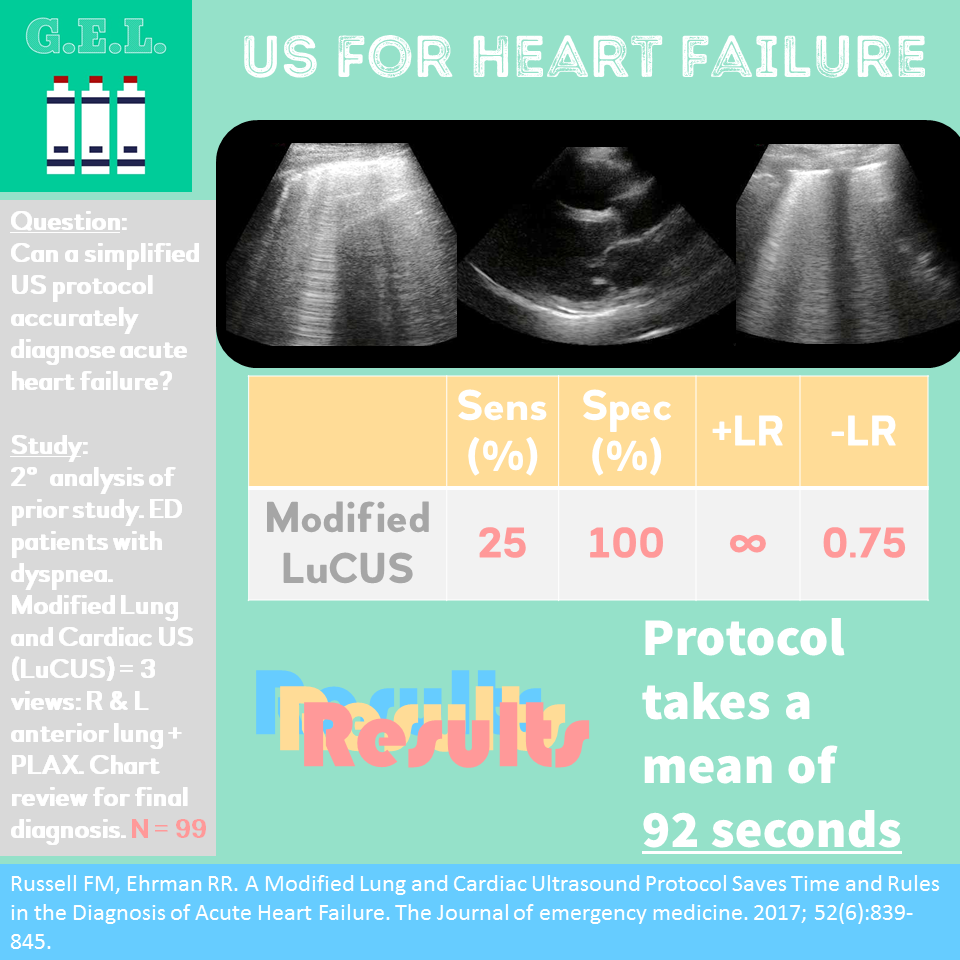
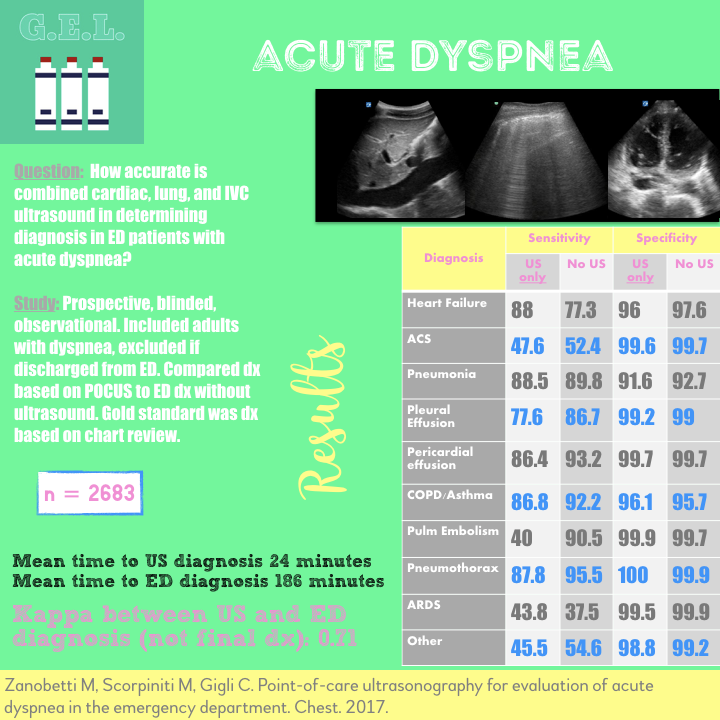
Heart Failure
Featured
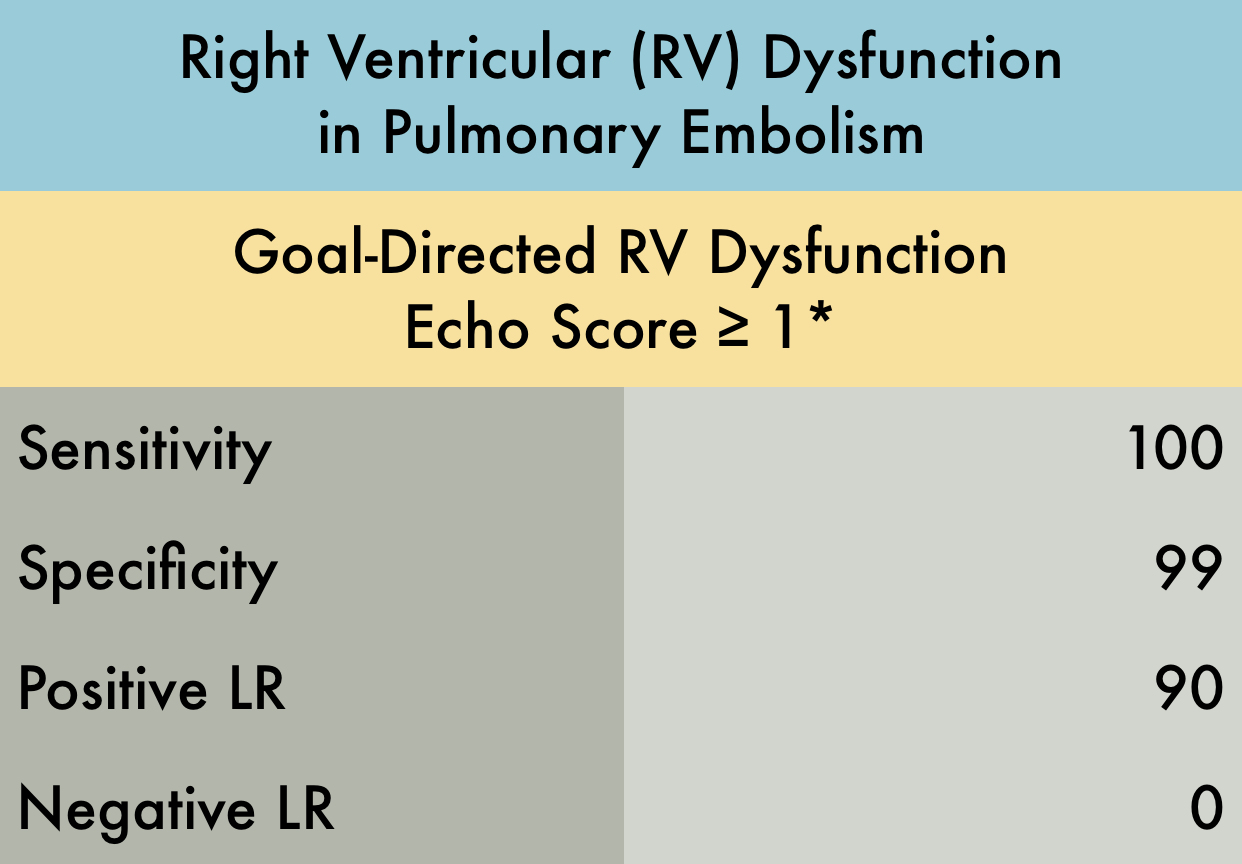
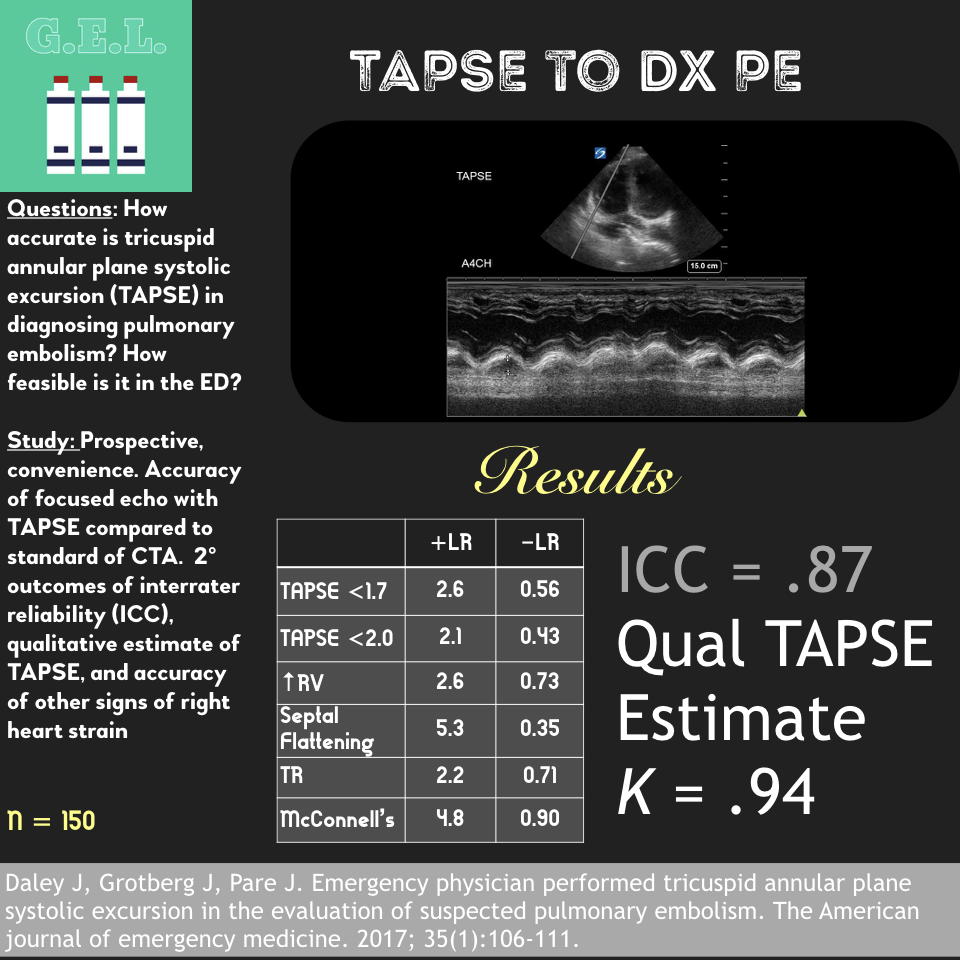
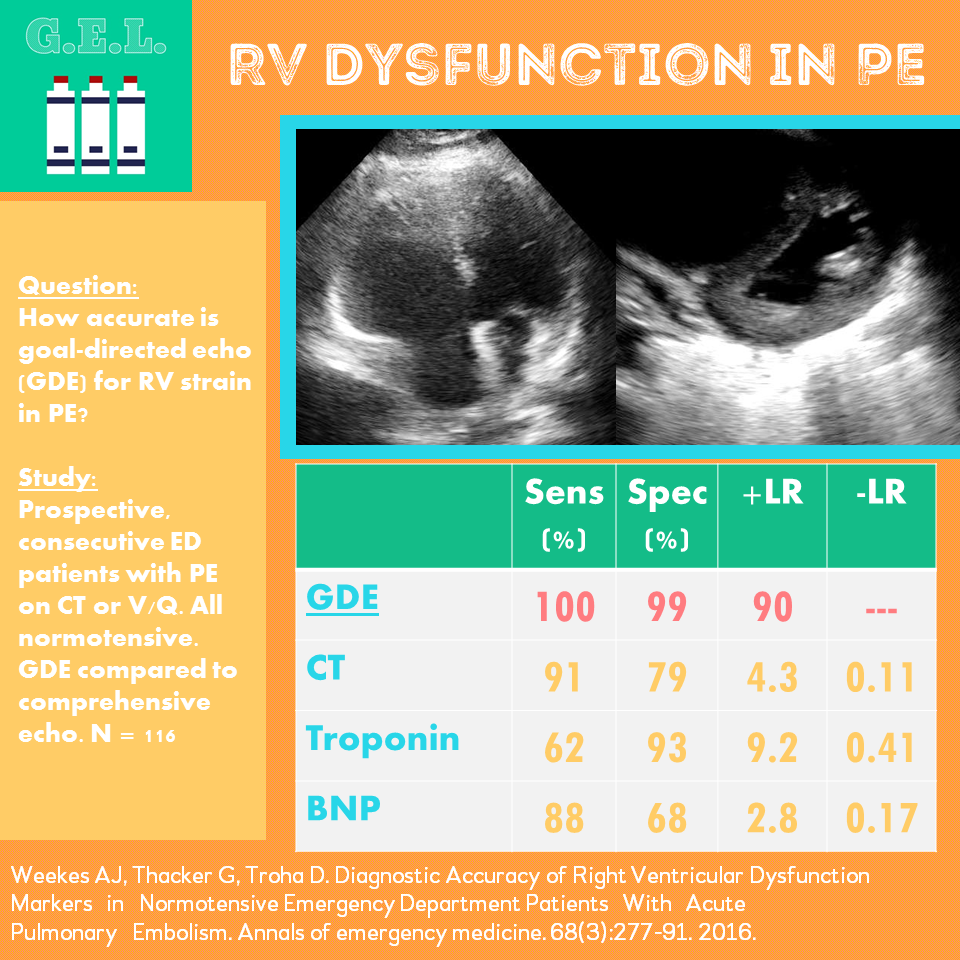
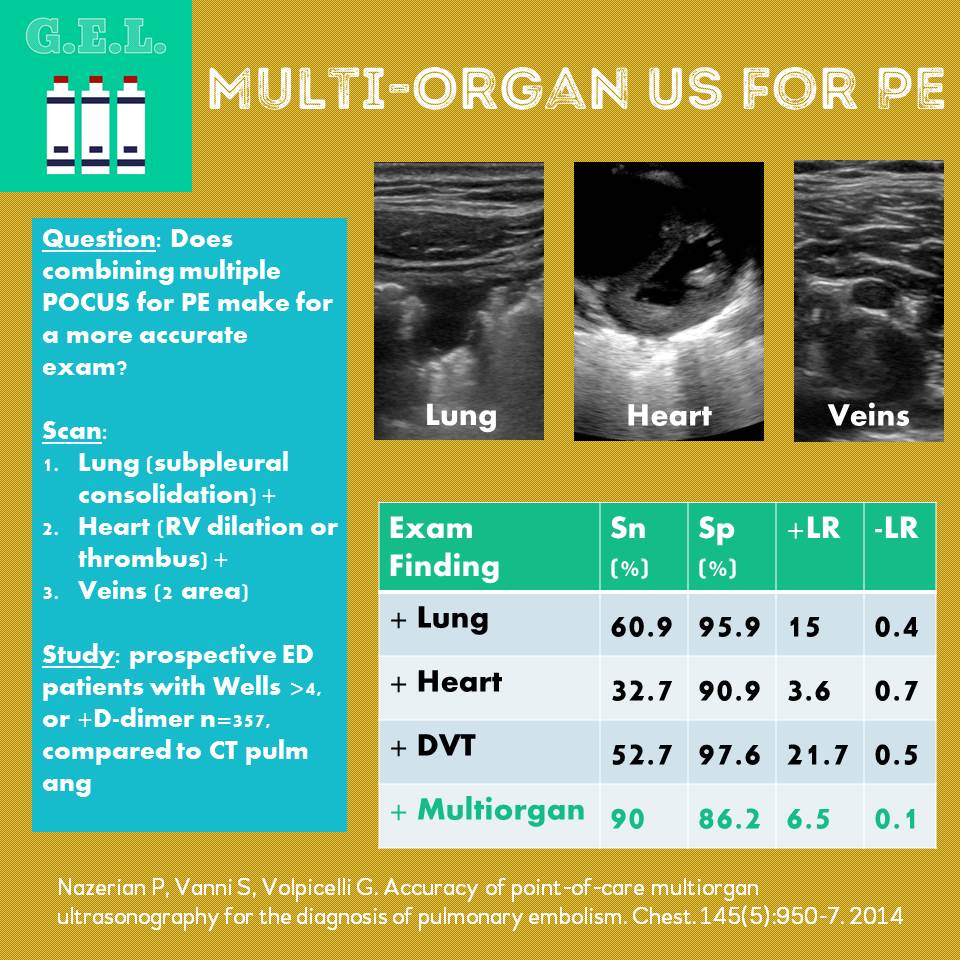
Pulmonary Embolism
Featured
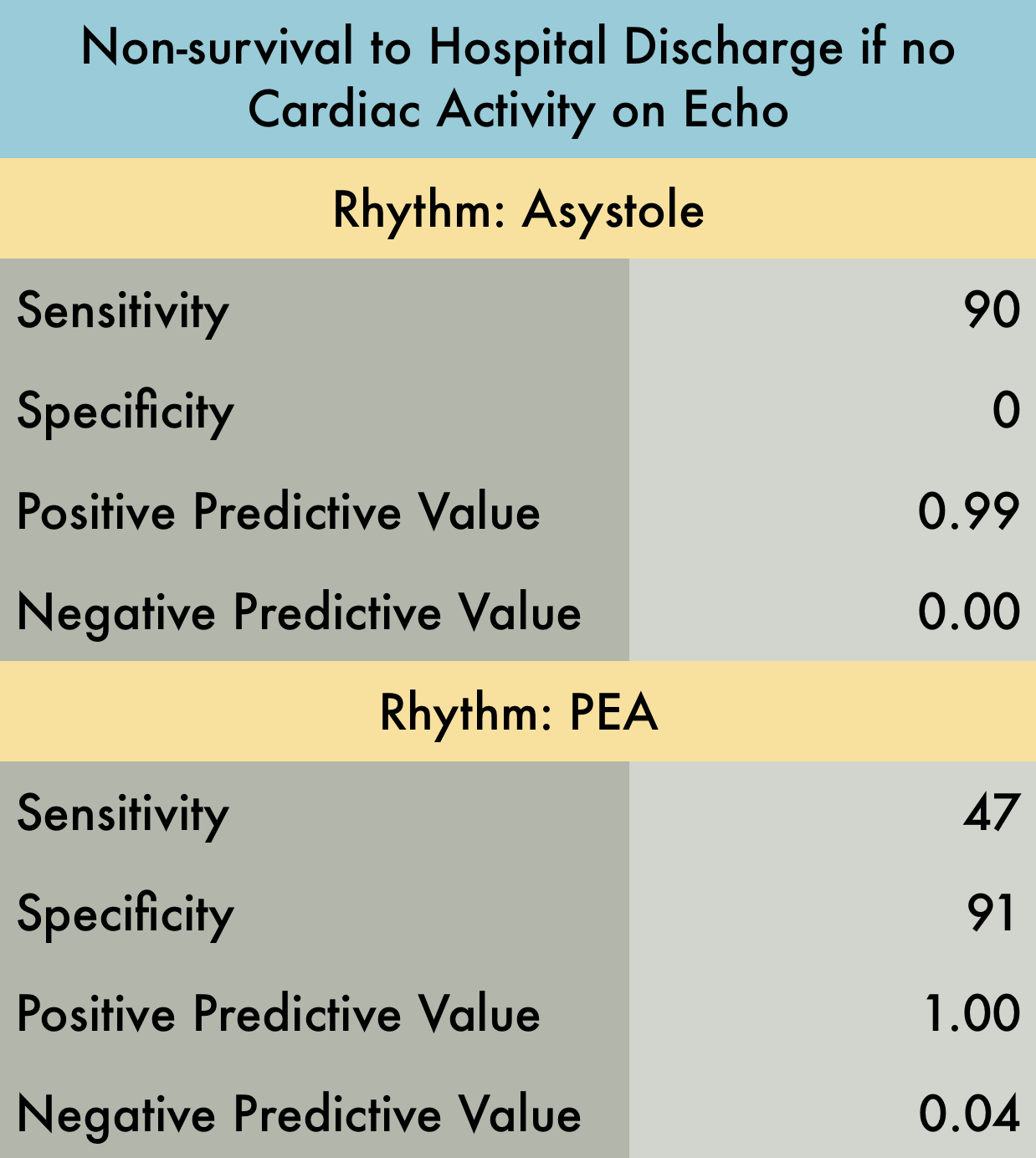
Cardiac Arrest
Featured
For more evidence check out our friends at US G.E.L.

Perfect your Echocardiography POCUS Technique with 5 Minute Sono